
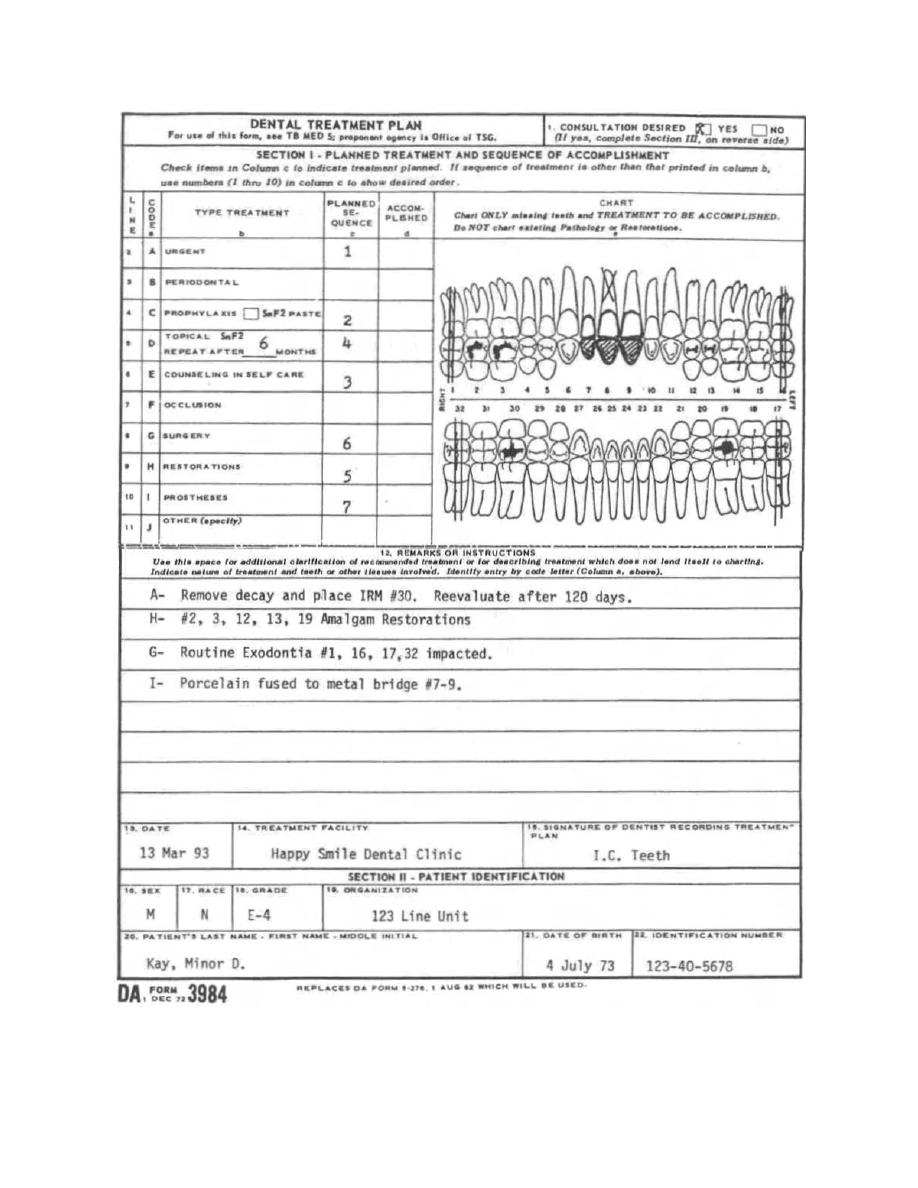
Proposed treatment plan dental form






DENTAL TREATMENT CONSENT FORM - DOC -.
Attending Dentist's Statement – Treatment Plan and Insurance ...
NationwideDentalPlan.com Multiflex indemnity dental insurance underwritten by Nationwide Life Insurance Company, individual and family dental insurance, dental plans
DENTAL TREATMENT PLAN CLAIM Verification No.: PART 1 - DENTAL ...
11.12.2008 · DP Family Care DENTAL TREATMENT CONSENT FORM Please read and initial the items checked below. Patient Name
07.07.2009 · DENTAL TREATMENT CONSENT FORM Please read and sign bottom of form Patient Name: _____ ____ 1. WORK TO BE DONE I understand that I am
Our Delta Dental Premier and Delta Dental PPO plans offer a higher level of coverage if you select an in-network dentist.
Attending Dentist's Statement – Treatment Plan and Insurance ...
Proposed treatment plan dental form
Nationwide Dental Plan - Indemnity Dental.
Dental Claim Form 1. Type of Transaction (Check all applicable boxes) EPSDT/Title XIX HEADER INFORMATION OTHER COVERAGE Statement of Actual Services – OR
Dental Treatment Consent Form (Confidential) . Patient Name: Please read and initial the items checked below and read and sign the section at the bottom ofthe form.
Dental Treatment Consent Form - Dr Chandra Williams Website
Treatment Options and Costs - Delta.
SI 3943 1 of 2 (4/09) Attending Dentist’s Statement Treatment Plan and Insurance Claim Report Standard Insurance Company Group Dental Insurance 800.547.9515 Tel 402
ANCILLARY CLAIM/TREATMENT INFORMATION - Encore Dental Insurance ...
Proposed treatment plan dental form
Dental Treatment Consent Form - Dr Chandra Williams Website
DENTAL TREATMENT CONSENT FORM Dentist’s Name_____ Patient’s Name:_____ Please read and initial the items
DENTAL TREATMENT CONSENT FORM
P A T I E N T P R O V I D E R I hereby assign my benefits payable from this claim to the named provider and authorize payment directly to him/her. Last Name Given
.
giorisjingna - 10. Dez, 03:01